
From Berth to Death
Flu kills. It kills even more when new technology changes everything.
Article body copy
US Navy soldiers lowered seven army coffins into the cold swell one by one. They said the names of the victims and a few words of solace. But they had other things to fret about as the Leviathan, queen of army transport ships, sped at 21 and a half knots on its way home to New Jersey—slowing down in U-boat territory was not an option.
The Leviathan was shuttling soldiers from the United States to Europe and had departed for its return voyage from France the previous day. It had left behind dozens more dead soldiers, none casualties of the war. They had died on the voyage over from North America, their war was with a deadlier foe: the greatest pandemic in modern history.
Ten days earlier, on September 29, 1918, the Leviathan had slipped its moorings in Hoboken, New Jersey, carrying over 9,000 army personnel bound for the killing fields of France. The most noteworthy passenger, however, was an influenza virus.
Many of the troops boarded with pounding headaches and sore throats. Some dropped listless on the dock before they reached the vessel. Ship doctors sent a few patients back to shore, but the war was more urgent than a coughing fit or a fever, and the crew set off as planned. Within 24 hours of leaving port, the virus had infected 700 troops and the sickbay was overflowing. Within a week, that number climbed to 2,000 as blood, vomit, and sputum coated the decks.

The Leviathan, overpacked with soldiers and crew members, ferried troops—and the influenza virus—between the United States and Europe during the First World War. Photo by Sueddeutsche Zeitung Photo/Alamy Stock Photo
Caregivers knew they had to separate the sick from the healthy, but on the Leviathan that proved impossible. The disease overwhelmed the bunk space. The Leviathan was a converted luxury liner designed to comfortably convey 6,800 souls, about twice the capacity of the Titanic. But the army had retrofitted the ship with stacked bunks and loaded it with 9,000 soldiers on top of the more than 2,000 crew. The airborne flu traveled with ease around the crammed ship. Harried staff tended to the sick lying on the decks and in the hallways: flu victims burning with fever and drowning from fluid-filled lungs.
An official military report on the voyage described the scene: “Pools of blood from severe nasal hemorrhages of many patients were scattered throughout the compartments and the attendants were powerless to escape tracking through the mess, because of the narrow passages between the bunks.”
The real horror of the outbreak aboard the Leviathan, though, was that it wasn’t an isolated event. Around the world, the same scene was playing out among soldiers and civilians, from isolated islands to teeming metropolises, from North America to Auckland, New Zealand. A horrifying flu had hit eerily fast and hard, striking the healthiest of people.
The pandemic, known as the Spanish flu, hit hardest from October 1918 to March 1919. Today we know that particular flu strain was more awful than usual. But its deadliness was amplified by crowded conditions, the ravages of war, and a revolutionary invention in maritime technology—steamships.
Steamships more than halved sailing times, carried more passengers than sailing ships, and more efficiently conveyed pathogens from one shore to another. Steamships spread the Spanish flu to almost every corner of the world carried in the lungs of sailors, soldiers, coal stokers, and civilians, infecting a third to half of the world’s 1.9 billion people and killing more than 50 million in six months. The death toll may have reached as high as 100 million over the course of the pandemic, but the chaos of the war and incomplete records cloud the true global impact. At the very least, influenza killed five times as many people as the First World War.

Like many infectious diseases, influenza capitalizes on overcrowded conditions, which it found on troopships during the First World War. Photo by American Photo Archive/Alamy Stock Photo
Since 1918, globalization has further shrunk the world. Today’s military carriers and cruise ships, not to mention airports and jetliners, struggle with their share of diseases like norovirus, but the flu remains a major candidate for a global pandemic. And in any pandemic, a critical variable is how fast the disease moves. As we grapple with the questions of if and how to monitor for diseases in today’s accelerated transportation networks—speed kills after all—what can we learn from the dark duet of the Spanish flu and steamships?
The Industrial Revolution radically altered life in the West. Nations focused on building factories, roads, railways, and cities. By the mid-19th century, everything and everyone moved faster and went farther. Railroads linked the once-remote edges of broad continents. But perhaps no technology affected the pace of living more than the coal-fired steamship. Replacing slow and often inefficient sails at sea, the steamship methodically contracted the world.
When the first steamships lumbered onto the waves in 1820, they were slow and clunky—not much better than sailing ships, which at the time took nearly a year to circumnavigate the globe. By the 1890s, steamships had reduced the journey to 100 days, and, since they were now cheaper to build and easier to run than sailing ships, they proliferated and soon dominated the seas. Plus, they could handle more cargo. Within decades, the volume of goods traded globally increased by a factor of six.
Improvement to steamships, such as lighter hulls and more powerful boilers, coupled with infrastructure projects like the first undersea telegraph cables and the Suez Canal in 1866 and 1869 respectively, made communication and trade between Asia and Europe effortless. British marine economist Martin Stopford says this connection had social impacts, particularly consolidating European empires. “The empires created a culture of continuous global travel,” Stopford says. This drastically increased the movement of people, military and civilian.
Epidemics have always followed maritime routes: the Black Death entered Europe via Italian ports, Captain Cook and other Europeans’ voyages introduced new and horrific venereal diseases to the South Pacific, and Irish emigrants fleeing the potato famine by ship were infamously riddled with typhus. Disease spread depends on variables such as infection rate, sanitation, contagion period, and available vectors, such as rats and fleas. Ships have all the right variables. Cram people close together, a few of them sick, and move them around quickly so they infect new people, and watch the magic unfold. It’s basic math.
From its inception, the steamship warped disease exchanges. Cholera, previously considered an Asiatic disease that only occasionally poked its nose into Europe, exploded along Mediterranean steamship trade routes in 1865. One astonished British doctor noted that the disease, while being no more deadly than previous outbreaks, had spread as far in six months as previous outbreaks had in two years. He wrote that “the unparalleled rapidity of progress finds no explanation in any peculiar virulence of the disease but solely … in the greater rapidity of traffic between different countries.” This became the new norm: even if a country got word of a disease outbreak on the other side of the world, it had less time to prepare than it had in the past since the infected could be days instead of weeks away.
By the time the Spanish flu virus emerged, just over 50 years after that worrisome speedy cholera, it found an even more developed transportation network connecting major cities around the world and growing networks in places such as the South Pacific that had never had consistent global transport links before. Moreover, at the start of the First World War in 1914, bigger and faster engines had reduced the journey time across the heavily traveled Atlantic from several weeks in the early days of steam travel to just five or six days.

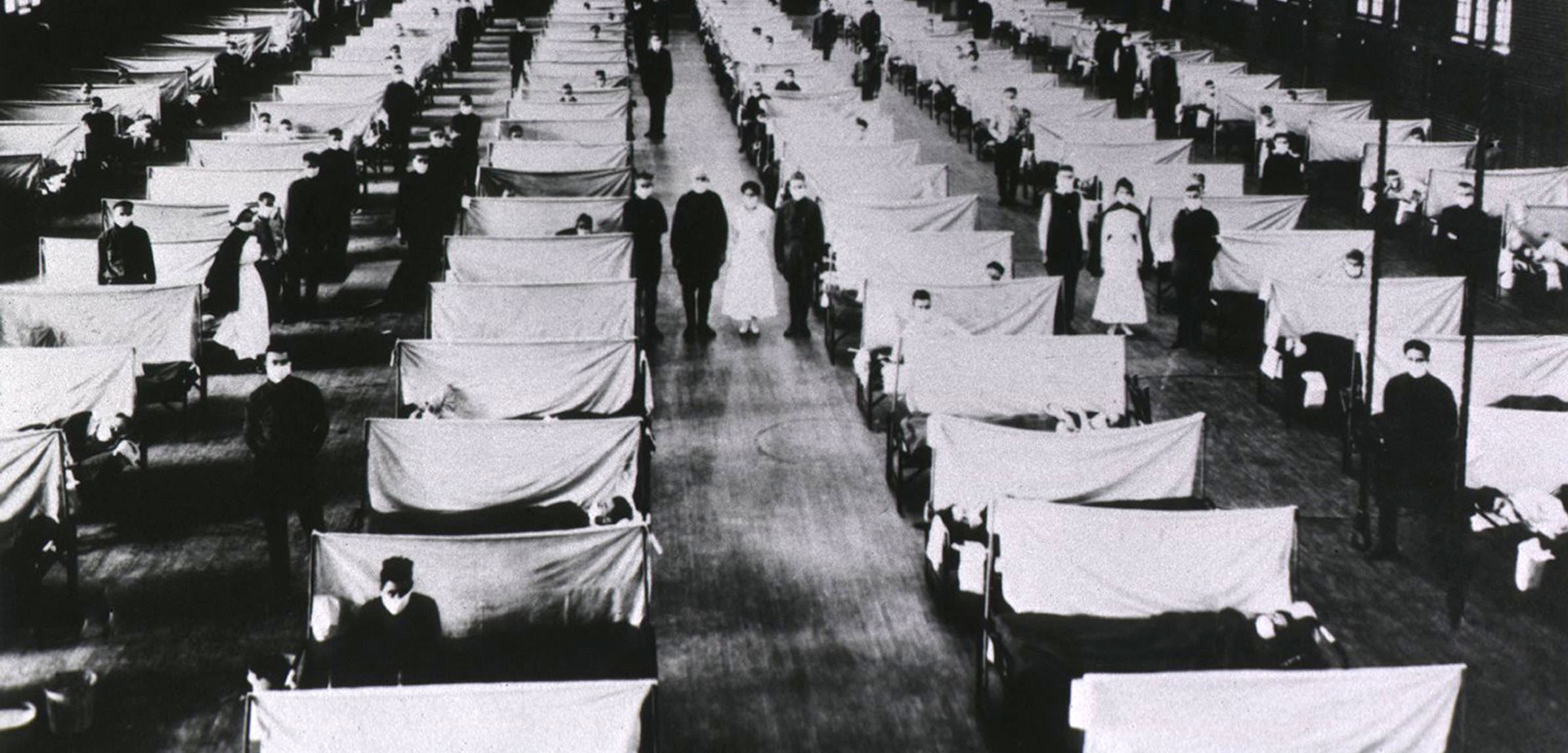
Red Cross staff in Washington, DC, demonstrated its preparedness at an emergency ambulance station during the 1918 influenza pandemic. The virus was so deadly, however, caregivers could do little more than offer comfort. Photo by Vintage Space/Alamy Stock Photo
Michael Worobey is an evolutionary biologist at the University of Arizona. He studies the evolution of flu viruses past and present. Before steamships, a flu virus could come on board a sailing ship making a transatlantic crossing but not survive to disembark. “It could move through the whole ship’s population and be gone by the time you get to the port four weeks later,” he says. “The steamship essentially allowed you to have a person who was infected when they get on and infected when they get off.” The virus never had a chance to burn out.
Still, amid the urgency of war, major medical authorities didn’t regard the flu as enough of a reason to quarantine a ship or close a port. The seasonal nuisance killed the vulnerable—mostly infants and the elderly—leaving the healthy with, at most, unpleasant aches and pains. There was, however, a foreshadowing of flu’s global potential in the steamship era: a Russian flu outbreak in 1890.
This outbreak was mild but spread fast. It reached the United States from Saint Petersburg, Russia, in 70 days, and traversed the planet in just four months. One British account noted, for example, that in Singapore the disease arrived via mail ships from Britain and other ports to the west. The sick spread the flu to wharf workers and from there the infection was passed from person to person. A 2010 study called the Russian pandemic the first to occur in a “highly connected world,” one linked by trains and steamships.
The globalness of the Russian and subsequent Spanish flu, Worobey says, was likely a result of steamships. “That was probably the first time in history where you could have, within a matter of a couple weeks, flu viruses that could get to pretty much every corner of the world,” he says.
The Russian flu killed around 300,000 (maybe more) people worldwide, which wasn’t enough to create a public health stir. A British report on the outbreak called influenza “a disease not indeed very fatal.” Even when Britain passed its Infectious Disease (Notification) Act in 1889, influenza was left off the list of a dozen or so culprits: only the traditional baddies like typhus, scarlet fever, and smallpox made the grade, and though there was some talk of adding influenza to the list in the 1890s, it never happened. The United States has required overseas consuls to report certain diseases since 1878, and within its own borders since 1893, but never flu.
Then came the First World War and a virus that suddenly mutated from seasonal nuisance to serial killer. In some cases, individuals died within hours of infection; in some small villages, particularly Indigenous communities in North America, most inhabitants succumbed. Nobody guessed the virus could do that, and the reasons why would remain murky for nearly a century.

In France, some soldiers fresh off ships from North America found themselves in an army hospital with the flu. Many died, never seeing combat. Photo by Everett Collection Inc/Alamy Stock Photo
Scientists have long speculated about what made the 1918 virus so lethal. “It was never clear why it was so virulent,” explains Darwyn Kobasa, a research scientist in the Zoonotic Diseases and Special Pathogens Division of Canada’s Public Health Agency. Kobasa has spent more than a decade studying the Spanish flu strain in a secure lab in Winnipeg, Manitoba.
Kobasa was part of a medical team that replicated the virus in 2004 using samples obtained from three exhumed 1918 flu victims. Kobasa and his coworkers inserted two genes of the deadly virus into a mild flu virus in mice. Those two genes helped the mild virus bind to the mice’s cells. All flu viruses have those two genes but the 1918 versions turned the mouse flu into an “ugly virulent virus in the mice,” says Kobasa. Something about that version was turbocharged. The mice’s immune systems went into overdrive, frantically responding to the pathogen, trying to eject it at any cost, wrecking tissues, burning energy, and even leading to secondary infections in the process. The virus turned the immune system into a biological saboteur.
In 2007, Kobasa went further and introduced the replicated 1918 virus to macaque monkeys whose immune systems more closely resemble humans’. The virus provoked the same strong immune response. In an echo of the past, the primates’ lungs filled with fluid and blood, an attempt to eradicate the pathogen. The virus kept on replicating even as the victims drowned. The blood and vomit that slicked the Leviathan’s deck wasn’t the result of flu, it was the response of the soldiers’ immune systems.
Intense crowding in ships and military camps may explain why the virus evolved into a killer, but the only thing everyone agrees on is that modern transportation was a huge factor in how quickly it spread, says Kobasa. “All of these changes in technology—the ability to move people everywhere and soldiers being housed in large camps where there was limited hygiene—all of these factors allowed the virus to spread so quickly.”
With all this hectic movement, no one’s sure where the whole thing started, but what is known is the pandemic had three waves. The second wave was responsible for the bulk of death and havoc, but the first arose almost half a year earlier when steamships journeyed from the United States to Europe.
The most widely cited origin theory posits that the epidemic first erupted at a US Army training camp called Camp Funston in Kansas. In January 1918, local hog farmers near the camp developed flu symptoms and some eventually died of pneumonia. The flu sickened the hogs as well.
Illness plagued recruits at Camp Funston into March. From Kansas, these recruits were transported to eastern ports and shipped off to France. Somewhere amid the trenches and overcrowded military camps of Europe, the virus mutated into an even more deadly viral force. (Its moniker, the Spanish flu, arose because Spain, not being involved in the war, didn’t censor reports of the pandemic for fear it would impact the war.) It then boomeranged back to North America in a second devastating wave, causing the bulk of the deaths and mayhem on both sides of the ocean in fall 1918, during a time of unprecedented troop movement. This story of Spanish flu’s emergence has been the narrative for decades.
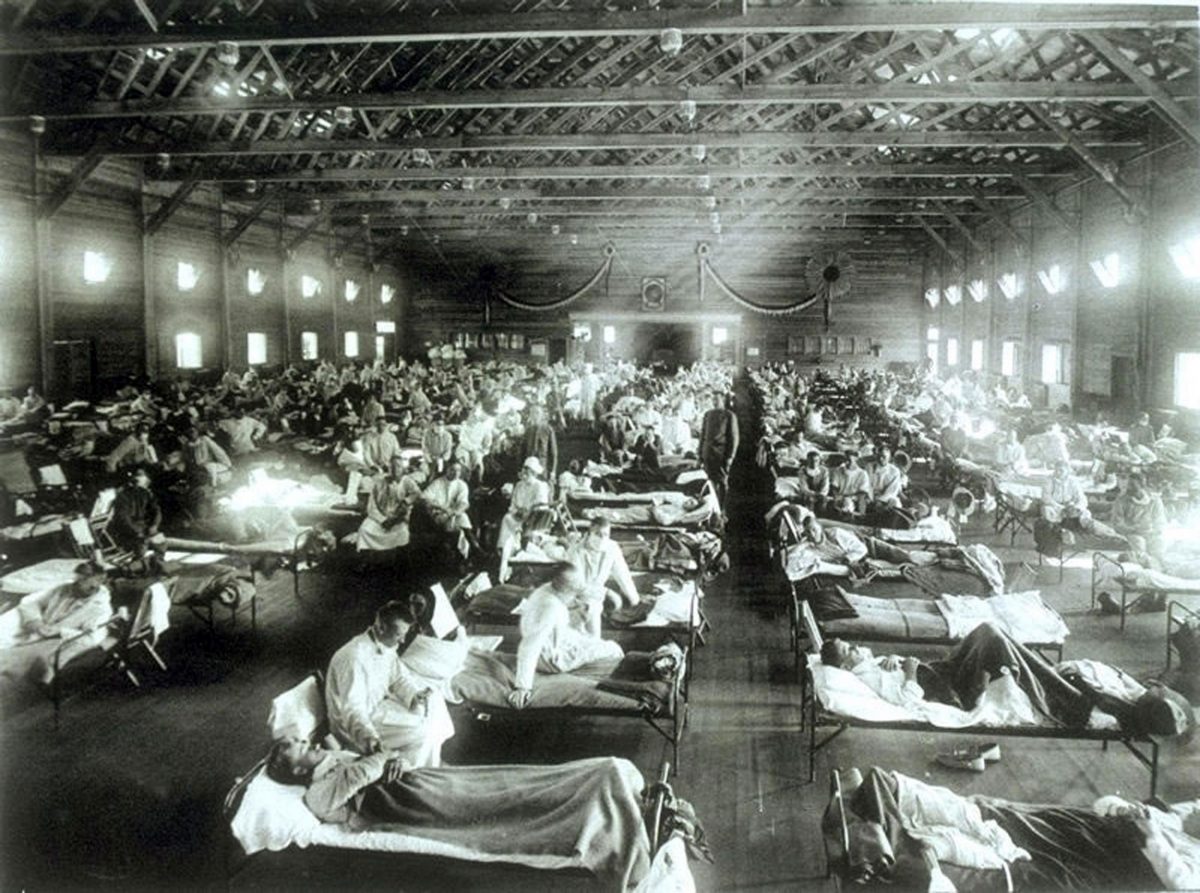
Images of sick and dying flu victims of the 1918 pandemic litter the historical record. The pandemic killed more people than the First World War. Photo by Science History Images/Alamy Stock Photo
Worobey, however, thinks the flu may have made its debut closer to the trenches. Étaples, a base for the front-line troops in northern France, was perfect for an outbreak with more than 100,000 people crowding the camp and its hospitals: ill soldiers with lungs compromised by deadly gas attacks and shipment after shipment of fresh troops.
Between December 1916 and March 1917, doctors at Étaples reported an unusual outbreak of influenza that attacked its victims so hard they turned blue with coughing. This was a whole year earlier than the flu at Camp Funston. Once the Spanish flu descended with surprising brutality in 1918, doctors who had treated the early cases in Étaples wondered if that halting first wave was a forewarning. They wrote to the medical journal The Lancet describing the flu as “fundamentally the same condition as the influenza pneumonia of this present 1918 pandemic.”
The doctors were witnessing the deadly second wave of the pandemic as it surfaced in three different military zones on three different continents. Crowded steamships connected all three centers of contagion.
In North America, Boston, Massachusetts, was a flu hotspot in August 1918—an outbreak was underway at Camp Devens outside the city. Designed for 36,000 men, the military camp housed 45,000. Navy personnel probably carried the virus to the Philadelphia Navy Yard, to Rhode Island, and by the steamship Harold Walker to New Orleans. From there, the virus spread westward and northward into one North American city after another.
In Europe, ports such as Brest, France, had steamship connections across the ocean, and also across the English Channel to the port of Plymouth, England, where the flu erupted as well. In August, the HMS Mantua, an armed merchant cruiser, left Plymouth and delivered the disease to what would be the third major epicenter, Africa.

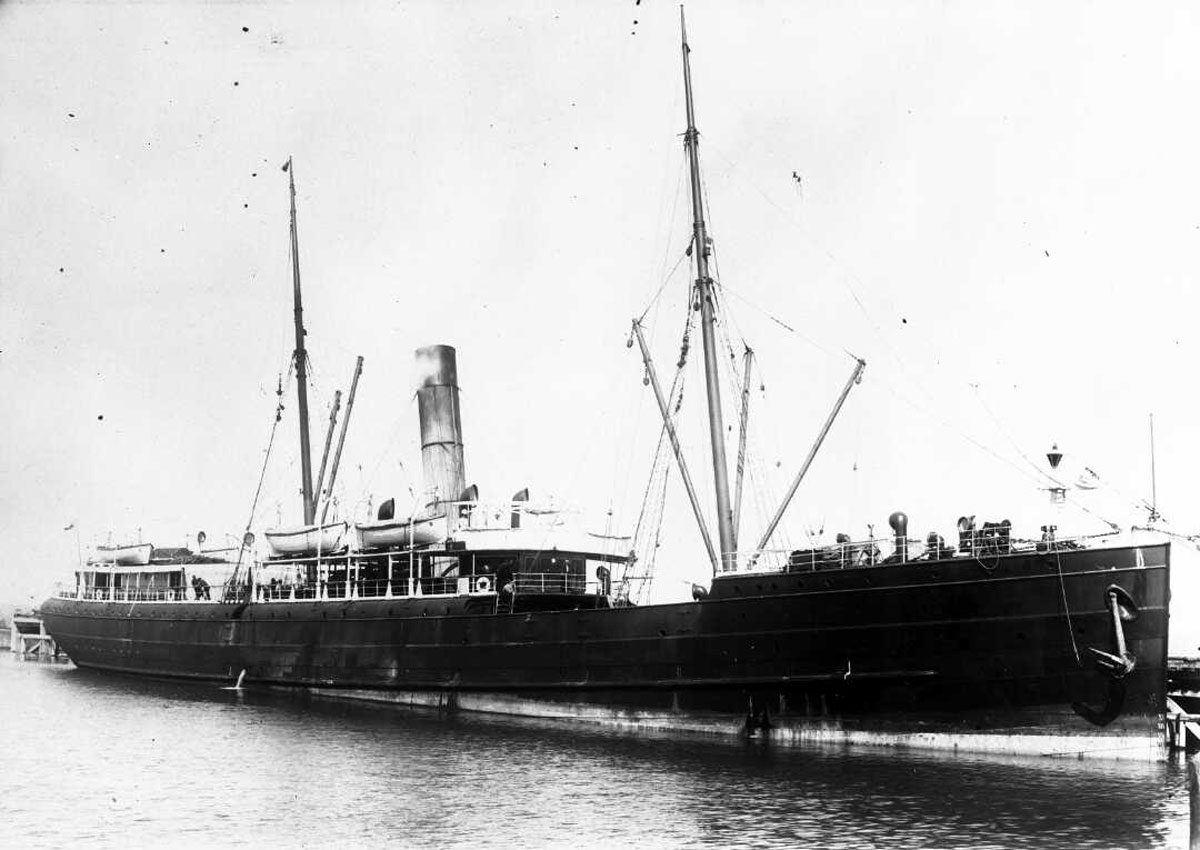
The HMS Mantua steamed from England to Africa, delivering troops and the influenza virus to a previously infection-free port. Photo by History and Art Collection/Alamy Stock Photo
Freetown, Sierra Leone, was a British colony and a major port on the continent’s west coast where ships refueled on their way to Asia. The Mantua arrived in Freetown with nearly 200 delirious sailors; 10 later died. The governor of the colony did nothing because influenza was not a reportable disease. Within two weeks, most of the city’s population was bedridden, while a ship that had stopped to refuel in Freetown brought the virus all the way to Cape Town, South Africa.
But perhaps the greatest medical holocaust in history happened in the South Pacific islands. Soldiers returning to New Zealand from Europe brought the second wave with them, and it hit Auckland in October 1918, killing 9,000 people over a two-month period. The pandemic spread out unevenly, devastating some communities and leaving others unharmed. The hardest hit overall were military camps. The disease expanded out from New Zealand onboard the SS Talune.
The Talune carried 175 passengers and a crew of 56. Every month before and during the war, it sailed out of Auckland to deliver mail and freight on a regular route. It sailed first to Fiji, where it took on laborers for a two-week circuit through Samoa and Tonga, before returning the workers home to Fiji and then steaming back to Auckland. But in late October 1918, the Talune steamed out of port for Fiji, carrying as many as five sick passengers. After a brief quarantine, the ship took on 90 Fijian laborers like always and headed off on its rounds.
The captain of the steamship SS Talune claimed he had no idea influenza was infectious. The result of his supposed ignorance was a cataclysmic infection rate on the island of Samoa. Photo courtesy of the Alexander Turnbull Library, Wellington, New Zealand. Ref: 1/2-080543-F.
The Talune docked in Samoa on November 7, 1918. Ironically, the former colonizer—Germany—had quarantined ships routinely. But the current New Zealand occupiers weren’t as punctilious, and at least half a dozen ill passengers walked ashore.
And then the dying began. “Every house was closed up with mats, and inside in the gloom the suffering of the inmates was pitiable to behold,” wrote one witness. “Some lay writhing on the ground, some were covered with mats, sweltering in agony beneath the covering; others lay in silence.” Over the following three months, Samoa suffered the greatest known proportional mortality of any state during the pandemic: 22 percent of the population died. The negligence in clearing the ship was so gross that New Zealand formally apologized to Samoa in 2002.
The dreadful voyage of the Talune also delivered the virus to Tonga, felling eight percent of the population. In contrast, the US-occupied colony of nearby American Samoa heard about the virus and imposed a strict quarantine on all ships and didn’t record one death from the 1918 influenza.
Ten days later, when the ship returned to Fiji, the 90 laborers, carrying the flu, disembarked to a crowded port: the war had ended on November 11 and celebrations had spilled out across the island. In the following weeks, the flu killed five to six percent of Fiji’s 163,000 inhabitants.
Steamships allowed influenza to spread around the globe more efficiently than ever before. Animation by Katrina Pyne
Why didn’t the authorities quarantine the Talune if they knew it had illness on board? Maybe ignorance was a factor but so was the economy. The steamship’s route and colonialism had connected these islands with a bustling global trade, and its timeline was driven by perishability. Two-thirds of the islands’ income came from exports, such as sugar and fruit. Any delay meant fresh food would rot and non-perishables would arrive late to New Zealand and Australia, and money would be lost. Quarantine now meant a serious economic hit. Again, steamships forged connections that the flu exploited mercilessly.
After the tragedy in the South Pacific, the flu surged again in a third and final wave in the winter of 1919. It continued the killing, albeit at more modest rates for a few more months. The final wave spilled into places that had so far remained relatively unscathed, including California and Australia, before finally burning out. More than a year after its genesis, the 1918 pandemic came to an end, leaving only corpses, grief, and some cruelly taught lessons for future generations.
The 1918 pandemic taught us that disease moves quickly and we should take the flu seriously—before people start dying. The flu is not on the World Health Organization’s reportable disease list: only yellow fever, plague, and cholera are. It’s up to individual countries, states, provinces, or cities to make their own lists of reportable diseases. (The United States has infant-related influenza and Canada has lab-confirmed influenza on their respective lists.) Yet the flu remains one of the most common infectious diseases on the high seas. The disease still plagues military vessels, cargo ships, and cruise ships. German researchers, for example, recently reviewed the medical logs of cargo ships. What they found was no surprise: flu outbreaks often sickened up to 41 percent of the crew.
It’s not just flu, of course. Cruise ships have become novel incubators for other infectious diseases, including the norovirus, an illness that leads to unforgettable bouts of explosive diarrhea and vomiting among passengers. The reason is, again, simple math. In the 1990s, the biggest cruise ship had capacity for 2,000 passengers, but newer ships now boast densities of over 6,000 all in the name of economics. In the past decade, the volume of human traffic on cruise ships grew from seven million tourists to 22 million.
A 2016 study in Nature declared the obvious about the health risks posed by these floating apartment buildings: “Long-term personal contact, complex population flows, a lack of medical care facilities, and defective infrastructure aboard most cruise ships is likely to result in the ship becoming an incubator for infectious diseases.”
These vessels not only pack large numbers of people together, but their passengers come from every corner of the globe. With each fresh batch of tourists exposed to infected crew or spaces, new microbial exchanges occur. Not surprisingly, cruise ships have hosted multiple outbreaks of flu over the past decade. On one cruise ship leaving Sydney, Australia, during peak flu season in 2000, 37 percent of 836 passengers surveyed after the trip had come down with the flu. Several had to disembark at the ship’s destination port of Nouméa, New Caledonia, before the return voyage and two died.
That’s worrisome considering cruise passengers’ demographics. The average cruise passenger in 2016 was 46, and there are still plenty of 55 plus cruises and senior discounts on major lines. So as a group, depending on the cruise, passengers can be more immunocompromised than the general population, just like gassed soldiers in the Western Front in 1918. Another lesson: be extra vigilant when it’s crowded and when people are weak.
Cruise ships also mix passengers from the southern and northern hemispheres, and as a result can change the timing of seasonal flu outbreaks, which traditionally strike as the weather gets cold. One group of travelers likely brought a flu from the southern hemisphere all the way to Alaska and Yukon in 1998. Over the summer, the virus may have infected more than 33,000 people.
Another lesson: diseases are tenacious stowaways that exploit ships’ broad travel itineraries and disembark in novel environments.
Over more than a century of epidemiological experiences, we should know by now how necessary it is to be cautious and vigilant—and how monitoring infectious diseases can avert disaster. But does the world have tools?
Worobey says there isn’t a comprehensive surveillance system that would catch new influenza outbreaks. The World Health Organization coordinates a network of national laboratories that can help detect if a new pathogen emerges, but many parts of the world (such as sub-Saharan Africa) aren’t sufficiently covered by this network. Further, surveillance is largely reactive not proactive. National science labs research the samples of pathogens that come from hospitals or doctors’ offices, only screening or sequencing a virus once lots of people fall sick. Take the 2015–16 outbreak of the Zika virus in the United States as an example: it reached Florida and Texas from an outbreak in Brazil from travelers who arrived on cruise ships and airplanes. Without anything in place to raise red flags when Zika first appeared, Worobey says the virus was probably circulating in the western hemisphere for more than a year before anyone noticed it.
“We’re always way behind the eight ball,” he says of pandemics. “It doesn’t have to be that way.” When it comes to influenza, he says that public health labs often only check the type of antigens to try to track what strains are going around. But they could track the source and spread of influenza outbreaks more accurately by taking it a step further and genetically sequencing the circulating viruses.
Worobey is a biologist now but he once worked as a forest fire fighter in British Columbia. He says that in that industry, monitoring for fires is a constant thing. Weather is monitored. Every lightning strike is triangulated. Flights are sent out at the first sign of smoke. He says it would be easy, albeit costly up front, to introduce a routine global monitoring system for influenza and other diseases, including reporting illnesses, sequencing virus samples, and tracking the first signs of trouble.
The world is more connected now than it was in 1918, and those connections are growing. Earlier this year, Qantas Airlines completed the world’s longest flight—just over 19 hours, New York to Sydney nonstop. In 2018, Royal Caribbean debuted the world’s largest cruise ship, Symphony of the Seas, a 6,800-capacity, 22-restaurant behemoth.
Pandemics will happen and from past experience we have good data on how they may unfold. Using this knowledge to spot the first signs of trouble would be a real shot in the arm for mitigating the effects.